
Clinical lab values help clinicians turn symptoms into measurable evidence about what is happening inside the body. A complete blood count, comprehensive metabolic panel, arterial blood gas, coagulation studies, and cardiac markers each reveal a different part of physiology. Together they help detect infection, anemia, electrolyte imbalance, acid base disorders, bleeding risk, organ injury, and myocardial damage.
Learning the major patterns makes it easier to connect numbers to real disease processes.
These tests are most useful when interpreted in context rather than as isolated values. CBC reflects blood cell production and immune response, CMP surveys electrolytes and organ function, ABG shows ventilation and metabolic status, coagulation studies assess clotting pathways, and cardiac markers identify heart muscle injury. Students should focus on normal ranges, what direction of change means, and how multiple abnormalities fit together.
Pattern recognition is especially important in emergencies such as sepsis, diabetic ketoacidosis, pulmonary failure, liver disease, and acute coronary syndrome.
Understanding Clinical Lab Values
A laboratory result is a measurement taken at one moment, not a diagnosis by itself. The body changes over hours and days, so trends often carry more meaning than a single result. For example, a falling hemoglobin level may point to active bleeding even when the first value was within the reference range.
White blood cell patterns matter too. Neutrophils often rise with bacterial inflammation, while lymphocyte changes can occur with many viral illnesses. A high white count does not prove infection.
Stress, steroid medicines, smoking, and bone marrow disorders can raise it. Red cell size helps narrow the cause of anemia. Small cells often fit iron deficiency or thalassemia.
Large cells can occur with vitamin B twelve or folate deficiency, alcohol use, liver disease, or some medicines. A reticulocyte count shows whether the marrow is responding by making new red cells.
The metabolic panel is best understood as a picture of water balance, kidney handling, and chemical reactions in cells. Sodium reflects the balance between body water and sodium more than total sodium stores alone. A low sodium level may result from excess water, certain medicines, heart failure, liver disease, or hormone problems.
Potassium deserves special attention because small changes can affect heart rhythm and muscle function. Kidney failure can raise potassium, while vomiting, diarrhea, or diuretic medicines can lower it. Creatinine rises when filtration by the kidneys falls, but it is influenced by muscle mass.
A small older adult may have important kidney disease with a creatinine that looks ordinary. Liver tests need careful naming. Some enzymes suggest injury to liver cells, while bilirubin reflects processing and excretion of a breakdown product from red cells.
Blood gas results show whether the lungs are removing carbon dioxide and whether the body has gained or lost acid. The body tries to compensate for a primary problem. In metabolic acidosis, the lungs usually respond with faster, deeper breathing to lower carbon dioxide.
In respiratory acidosis, the kidneys retain more bicarbonate over time, though this response is slow. Compensation reduces the pH change but usually does not fully correct it. Oxygen values require extra caution.
A sample labeled arterial but actually drawn from a vein can give misleading oxygen results. Pulse oximetry estimates oxygen saturation, yet it does not show carbon dioxide retention or the full acid base state. This matters in conditions such as severe asthma, chronic lung disease, opioid overdose, and diabetic ketoacidosis.
Clotting tests are strongly affected by medicines and by how the sample was collected. Heparin can prolong activated partial thromboplastin time, while warfarin commonly raises INR. Liver disease may prolong several clotting tests because the liver makes many clotting factors.
A low platelet count creates bleeding risk through a different mechanism than missing clotting factors, so both platelet number and clotting times matter. Cardiac markers must be interpreted with symptom timing and repeated measurements. Troponin can rise after reduced blood flow to the heart, yet it may rise in kidney disease, severe infection, rapid heart rhythms, or inflammation of heart muscle.
A rising or falling pattern is often more informative than one elevated value. Students should first identify what each test measures, then connect it to the patient story, medicines, timing, and related results.
Key Facts
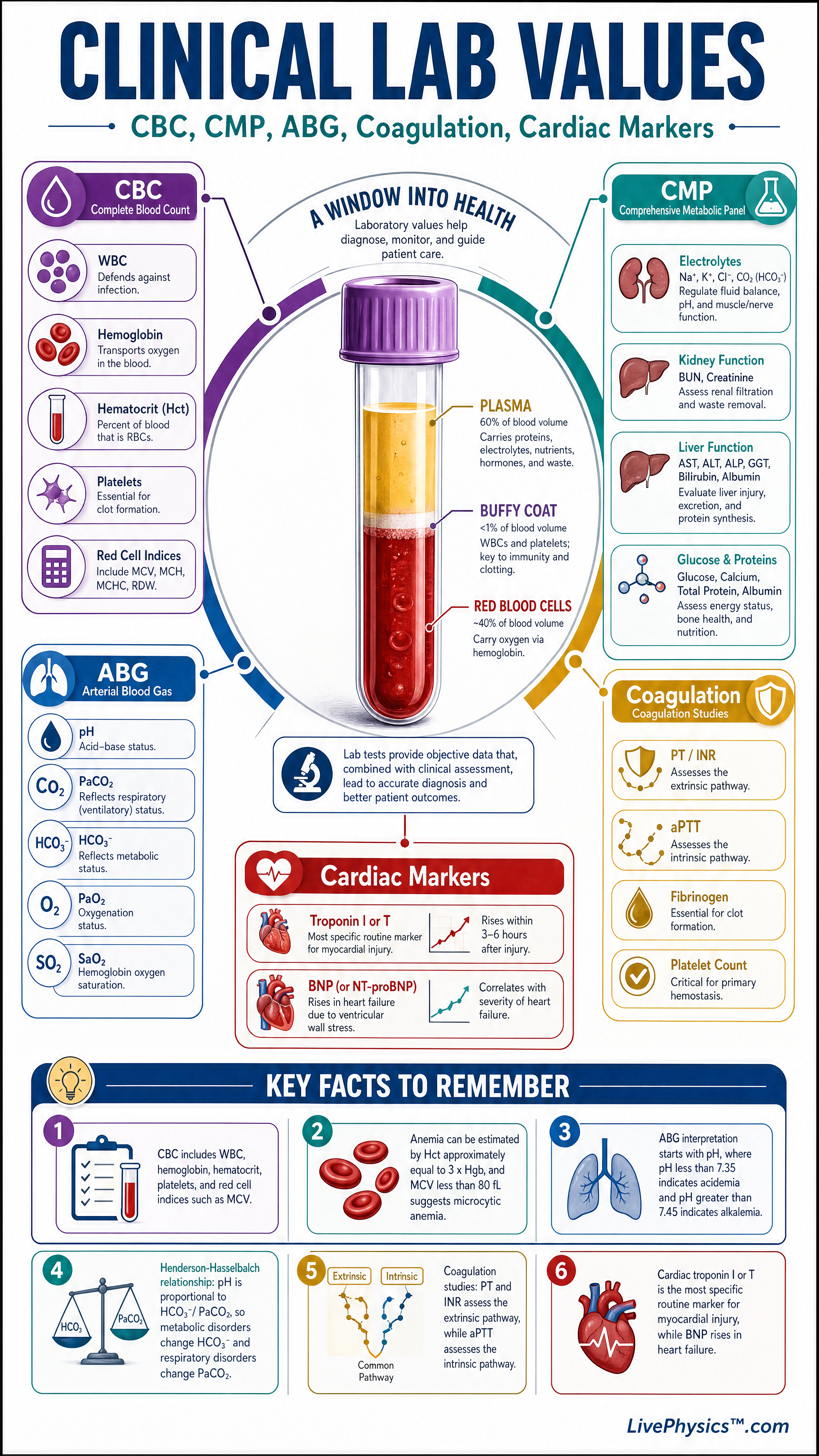
- CBC includes WBC, hemoglobin, hematocrit, platelets, and red cell indices such as MCV.
- Anemia can be estimated by Hct approximately equal to 3 x Hgb, and MCV less than 80 fL suggests microcytic anemia.
- ABG interpretation starts with pH, where pH less than 7.35 indicates acidemia and pH greater than 7.45 indicates alkalemia.
- Henderson-Hasselbalch relationship: pH is proportional to HCO3-/PaCO2, so metabolic disorders change HCO3- and respiratory disorders change PaCO2.
- Coagulation studies: PT and INR assess the extrinsic pathway, while aPTT assesses the intrinsic pathway.
- Cardiac troponin I or T is the most specific routine marker for myocardial injury, while BNP rises in heart failure.
Vocabulary
- Hemoglobin
- Hemoglobin is the oxygen carrying protein in red blood cells and is used to assess anemia or blood loss.
- Creatinine
- Creatinine is a waste product filtered by the kidneys and is used as a marker of renal function.
- PaCO2
- PaCO2 is the partial pressure of carbon dioxide in arterial blood and reflects how well the lungs are ventilating.
- INR
- INR is a standardized measure of prothrombin time used to compare clotting function across laboratories.
- Troponin
- Troponin is a protein released into the blood when cardiac muscle cells are injured.
Common Mistakes to Avoid
- Memorizing single lab values without looking for patterns, because many diagnoses depend on combinations such as low pH with low HCO3- or chest pain with rising troponin.
- Confusing serum potassium with total body potassium, because a normal or high blood potassium can still occur when total body stores are depleted, especially in acid base disorders.
- Interpreting a normal early troponin as ruling out myocardial infarction, because troponin often rises over time and must be correlated with symptoms, ECG findings, and repeat testing.
- Mixing up PT and aPTT pathways, because PT and INR mainly reflect the extrinsic pathway while aPTT mainly reflects the intrinsic pathway.
Practice Questions
- 1 A patient has Hgb = 8 g/dL and MCV = 72 fL. Is the patient anemic, and is the anemia microcytic, normocytic, or macrocytic?
- 2 An ABG shows pH = 7.30, PaCO2 = 50 mmHg, and HCO3- = 24 mEq/L. Is this primarily respiratory acidosis, respiratory alkalosis, metabolic acidosis, or metabolic alkalosis?
- 3 A patient with chest pain has a normal CBC and CMP but a rising troponin on repeat testing. Explain why the cardiac marker is more clinically important here than the normal blood count and metabolic panel.